14 YEAR OLD MALE WITH PERIPHERAL CYANOSIS
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CHIEF COMPLAINTS:
C/O • FEVER since 3 days
• LOOSE STOOLS since 3 days.
•VOMITING since 3 days.
• bluish discoloration of fingers of upperlimb simce yesterday.
History of present illness:
Patient was apparently asymptomatic 3 days back then he developed
Fever, which is high grade fever, not relieved on taking medication.
Loose stools, 3-4 episodes/ day till yesterday.
H/O 3 episodes of vomiting on day 1, which is bilious, non projectile.
Associated with head ache in occipital region since 3 days.
• from yesterday patient developed bluish discoloration of fingers.
PAST HISTORY:
Not a known case of, hypertension, diabetes,CAD, EPILEPSY, ASTHAMA.
H/O injury to index finger and surgery done to finger at 1 year of age.
FAMILY HISTORY:
NO SIMILAR COMPLAINTS IN THE FAMILY.
Personal history:
Diet- mixed
Appetite- normal
Bowel and bladder movements- Regular
Allergies- No
Addictions- No
GENERAL EXAMINATION:
Pt is conscious, coherent and cooperative
At the time of presentation hand and feet are cold compared to forearm.
CYANOSIS - PRESENT


No pallor, no icterus, , no clubbing, no lymphadenopathy.
VITALS- day 1
TEMP-101.4 F
BP-100/60
Pulse rate-86bpm
RR- 18cpm
SYSTEMIC EXAMINATION:



ABDOMINAL EXAMINATION:
Umbilicus inverted , No abdominal distention,no visible pulsations,scars and swelling.
PALPATION: Soft, non tender, no organo megaly.
AUSCULTATION:
BOWEL SOUNDS HEARD
Cardio vascular examination:
No visible pulsations, scars, engorged veins. No rise in jvp
Apex beat is felt at 5 Intercoastal space medial to mid clavicular line.
S1 S2 heard . No murmurs.
Respiratory system : Shape of chest is elliptical, b/l symmetrical.
Trachea is central. Expansion of chest is symmetrical
Bilateral Airway Entry - positive
Normal vesicular breath sounds
CNS EXAMINATION:
No signs of meningeal signs
Cranial nerves: normal
Sensory system: normal
Motor system: normal
Reflexes: Right. Left.
Biceps. ++. ++
Triceps. ++. ++
Supinator ++. ++
Knee. ++. ++
Ankle ++. ++
Gait: normal.
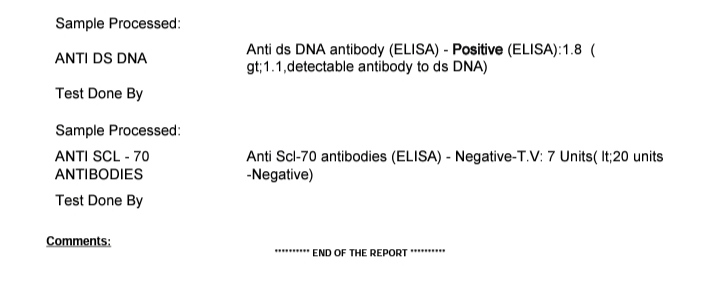
INVESTIGATIONS:










DIAGNOSIS: Acute Gastroenteritis,Peripheral cyanosis(1episode-Resolved) with cervical lymphadenopathy.
Treatment:
1. Tab. Paracetamol PO/TID
2. Temperature monitoring 4th hourly.
Day 3
AMC
14/M
S- Loose stools decreased.
O-
Patient is conscious coherent and cooperative
BP- 100/60mm hg
PR- 98 bpm
RR- 18cpm
TEMP-101.4 F @ 8 am
SpO2- 99% on RA
CVS-S1S2+
R/S-BLAE+, NO ADDED SOUNDS.
P/A-soft , non tender
CNS-NFND.
Diagnosis: Acute Gastro enteritis,peripheral cyanosis(1episode-Recovered),Generalised Lymphadenopathy
Treatment:
1. IVF NS, RL @100 ml/hr
2.TAB PCM 650MV PO/TID
3.TEMPERATURE MONITORING 4TH HOURLY
AMC bed 1
Day 4
S-complaints of loose stools subsided
C/o one episode of vomiting (no food particles) yesterday night
Fever spikes @4pm 103F
@12am 101.6F
O-
Patient is conscious coherent and cooperative
BP-90/60mmHg
PR-92bpm
TEMP-98.4F
SPO2-96% at RA
GRBS-104mg/dl @8AM
CVS-S1S2+
R/S-BAE+,NVBS-heard
P/A-soft and mild tenderness in umblical region, no organomegaly
CNS-NFND
A-
ACUTE GE with PERIPHERAL CYANOSIS ( 1episode -resolved ) with GENERALISED LYMPHADENOPATHY
P-
1.IV FLUIDS @NS RL @100 ml/hr
2.TAB.PCM650mg PO TID
3.INJ.MONOCEF 1gm IV BD
Urine and blood cultures negative
Day 5
S- C/O loose stools 4 episodes in 4-7 pm yesterday
1 episode today morning
O-
Patient is conscious coherent and cooperative
BP-90/60mmHg
PR-84bpm
TEMP-100.1F
SPO2-96% at RA
GRBS-103mg/dl @8AM
CVS-S1S2+
R/S-BAE+,NVBS-heard
P/A-soft and no organomegaly
CNS-NFND
Urine and blood cultures negative
A-
ACUTE GE with PERIPHERAL CYANOSIS ( 1episode -resolved ) with GENERALISED LYMPHADENOPATHY
P-
1.IV FLUIDS @NS RL @100 ml/hr
2.TAB.PCM650mg PO TID
3.INJ.MONOCEF 1gm IV BD
Day 6:

























































Comments
Post a Comment